Разработка ПО
Разработка ПО
 Менеджмент
Менеджмент
 Для компаний
Для компаний
 Для стартапов
Для стартапов
 Архитектура ПО
Архитектура ПО
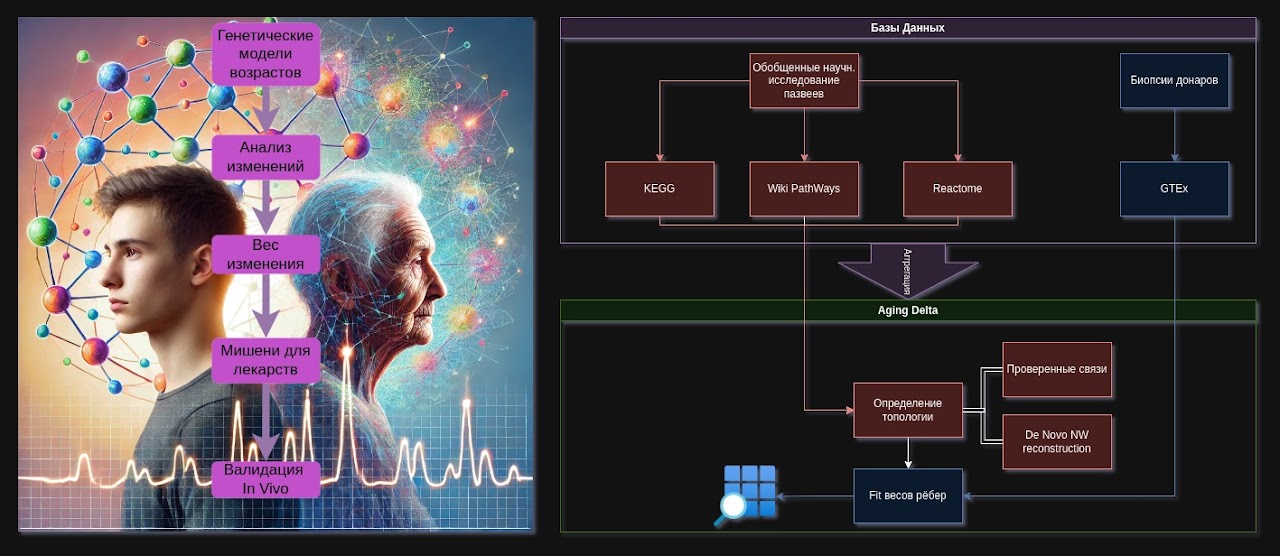
Recently I met with the head of a network of boarding houses. It was not just another business meeting, but a new puzzle piece in my unified picture of the world. The boarding houses provide geriatric services — they help elderly people not merely live out their remaining years, but LIVE their golden age. The project we discussed covers not just accounting and monitoring. It covers social norms, standards, legislative apparatuses, and regulations on a state scale. A year earlier, I met the head of the epigenetics department of the Kyiv Institute of Gerontology, and we started a project with them to compare expressions in the genome of young and elderly people based on a biopsy database. And the puzzle pieces began to form a more connected picture. In this article I will explain how I see the connection between my work — designing architecture for software systems — and immortalism, gerontology, and geriatrics.
Оглавление
Immortalism you would not be ashamed to sign
Would you like to live better and longer? A rhetorical question. Well, anyway...
Every IT project, every application and corporate software is a step toward eternal life if its structure is endowed with sufficient resilience and is capable of existing and developing long-term, for generations. These are exactly the systems we strive to design and program. But we will discuss next time how automation leads to longevity, and now let us honestly talk about the core of the real subject area that is capable of ensuring long-term life for the human individual himself.
Immortalism is usually sold as a beautiful fairy tale: eternal youth, consciousness upload, cryochambers, nanorobots. This is a problem. Because against this futuristic background, real old age looks like something obvious, boring, and secondary. Aging people turn into statistics and a "side effect", not the foundation of the solution.
If we think seriously, immortalism can hardly begin and develop in metaverses. It begins in geriatrics — where aging has already happened, where biology behaves honestly, without sci-fi makeup. But geriatrics in its current form does not lead us to immortality. Gerontology without a living, systemic clinical field does not either. So the task is not to “believe in eternal life”, but to build an infrastructure where:
- an elderly person receives higher-quality, humane, transparent care,
- the system collects correct data about aging in the process,
- gerontology receives material for work,
- society receives tools for the consistent extension of healthy life,
- and all this is not in conflict with ethics, but based on it.
Below is what such a connection may look like.
Three levels: subject, model, philosophy
- Geriatrics is the practical medicine of the aging person. Pain, weakness, comorbidities, falls, loneliness. The harshest, least pretty, and most honest level.
- Gerontology (including epigenetics, molecular aging, markers, interventions) is the level of mechanisms. Why cells give up, what breaks in immunity, what happens to gene expression, how this can be slowed down.
- Immortalism is not the religion of “we will live forever”, but a target framework: the consistent reduction of the probability of death from manageable causes and the extension of healthy life as far as technologies allow.
Right now these three levels live disconnected. Immortalism talks about the future, gerontology talks about markers, geriatrics talks about a shortage of caregivers. The connection is possible only through structure.
Standards as a bridge: how geriatrics becomes a source of progress
The key idea: geriatrics stops being a “dumping ground for incurable cases” and turns into a standardized research-clinical network.
What this means in practice:
- Standardized diagnostics and monitoring.
- Unified examination protocols are introduced for geriatric patients: baseline panels, cognitive status, functional tests, inflammation markers, and (where available) epigenetic and metabolic profiles.
- Data is collected in a unified format suitable for analysis, not as scattered PDFs.
- Legally and ethically verified access to data.
- The patient is told in advance: your information (anonymized) may become a contribution to aging research.
- Transparent consent forms: one can agree only to the use of data, one can agree to a biobank, one can agree to participation in mild observational studies.
- No “you are old anyway, so it does not matter” — only voluntariness, only with clear consciousness.
- Financial motivation of the system.
- The state and foundations distribute subsidies/grants not simply “for beds and food”, but to geriatric institutions that comply with standards:
- quality of care,
- completeness and correctness of data,
- participation in clinical and observational programs.
- The better a clinic works according to the standard (both for the patient and for science), the easier it is for it to attract funding.
- The state and foundations distribute subsidies/grants not simply “for beds and food”, but to geriatric institutions that comply with standards:
- Biobanks without torture.
- This is not about “harsh experiments”, but about reasonable integration:
- additional blood tubes during scheduled tests,
- biopsies only where they are clinically justified,
- long-term observation (dynamics of markers, response to therapy).
- This turns geriatrics into a legitimate source of real data about aging — not an experiment on the vulnerable, but a platform for cooperation.
- This is not about “harsh experiments”, but about reasonable integration:
This is how a two-way connection is born: geriatrics gives gerontology numbers and tissues; gerontology returns protocols to geriatrics that actually improve quality of life.
Problems with this logic — and solutions
Problem 1. The risk of exploiting the elderly “for science”.
Solution:
- A strict ethical framework: independent oversight boards, multi-stage informed consent.
- A ban on hidden coercion: participation in research cannot be made a condition for receiving basic care.
- A positive incentive: participants receive priority access to better diagnostic and rehabilitation protocols, but basic care does not depend on consent.
Problem 2. Data infrastructure.
Solution:
- Creation of open (with anonymization) national/international aging registries: clinical indicators, markers, treatment outcomes.
- Common standards for different clinics and countries: unified formats, APIs, quality audit.
- Access for universities and laboratories through transparent competitions, not backroom arrangements.
Problem 3. Motivation of doctors and clinics.
Solution:
- Money is tied to standards and participation in programs (pay for quality, not for the “number of days spent lying in bed”).
- Training geriatricians as a key profession of the future: they do not just “treat old people”, they stand at the forefront of the fight against aging.
- Reputational capital: clinics that become “longevity centers” receive status, personnel, and resources.
Problem 4. The gap between “treating old age” and “immortalism”.
Solution:
- Clearly define the trajectory:
- Phase 1: humanization and standardization of geriatrics.
- Phase 2: systemic data collection and analysis → identification of reproducible targets.
- Phase 3: mild interventions in geriatrics (combinations of already approved drugs, regimens, nutraceuticals, technical support).
- Phase 4: transfer of effective interventions to earlier age groups as prevention.
- Phase 5: formation of a set of methods that measurably reduce biological age and risks — not with slogans, but by survival curves.
This is no longer fantasy immortalism, but engineering immortalism.
How “reasonable immortalism” grows out of this
If we remove the noise, immortalism in a practical sense is:
- refusing to accept aging as a “norm that must not be touched”;
- the development of long-term infrastructure where each iteration improves:
- the lives of the current elderly,
- the quality of data about aging,
- tools for the next generation.
The connection works like this:
- Geriatrics gives us a real map of the battlefield: what exactly breaks and how it looks not in theory, but in people.
- Gerontology on this basis stops being a “game with markers for the sake of articles” and becomes a supplier of concrete, verifiable interventions.
- Immortalism becomes not a promise of “eternal life”, but a requirement for the system:
- any new technology must be embedded into this connected network;
- evaluated by its impact on life expectancy and quality of life,
- developed according to the principle: less pain now, more control tomorrow.
An elderly person in such a model is not an object of pity and not a test subject, but a full partner: a carrier of data, experience, and will, who consciously decides to help future generations. And the system responds honestly: for your contribution, we give you better access to care, transparency, and respect.
Instead of a conclusion
Practical immortalism begins not with the statement “we will defeat death”, but with reforming how we treat old age today.
Geriatrics as infrastructure.
Gerontology as mechanism.
Immortalism as vector and criterion.
Everything else is science fiction that we will be able to afford only after we learn to work properly with those who are aging here and now.
PS: As for science fiction and futurism, the site describes our experience developing and launching a large project for digitizing cemeteries with artificial intelligence and a modern generator of the "internet for the departed" based on AI — later I will separately tell the continuation of this philosophy, which begins with eternal memory and currently ends with the barely, barely science-related process of reviving deceased people (I emphasize once again — this is futurism, at best it is a philosophical vector, very far from the current capabilities of science). And for the manifesto of the full chain of mad views from global automation to eternal life with the generation of one's own isolated worlds and the study of the foundation of current reality — read the manifesto at ingello.com